
Pancreatic Lesions
What are pancreatic lesions?
Pancreatic lesions are abnormalities in the pancreas which are often seen on scans. They represent an area where the tissues are different from the rest of the pancreas. These may be cysts, tumours or localised areas of inflammation.
Are all pancreatic lesions bad news?
Not necessarily. Some of these lesions may be entirely benign, with no possibility of turning malignant (“cancerous”), whereas others may be cancerous. Pancreatic lesions can be largely divided into those which are cysts (= fluid filled) or those which are solid.
What if I had a solid lesion in the pancreas?
The major worry about a solid lesion is that it could be a pancreatic cancer. Unfortunately, there is no test which can 100% rule out cancer. Even a biopsy can falsely report benign disease in a patient with pancreatic cancer. Therefore, when a solid lesion is found in the pancreas, there is often a good argument for the surgical removal of this lesion. Clearly, this is not the case for all patients, but surgery would usually be on the cards. In difficult cases, the patient’s case may be discussed in a multidisciplinary meeting (MDT) to gather different opinions on the case.
What if it were a cystic lesion?
There are many different types of cysts in the pancreas. It may range from the benign serous cystic neoplasm to a premalignant lesion (IPMN) to a cystic type of pancreatic cancer. Because of this, the management of pancreatic cysts require careful investigation. Depending on the cause, the management may vary from a “watch and wait” approach to recommendation for surgical removal.
How can one differentiate between the different possible diagnoses?
The most important investigation in determining what a pancreatic lesion represents is a good quality scan (CT or MRI) of the pancreas. These special scans require the use of a dye, which is injected into a vein in the arm. As the tumour and the rest of the pancreas have different amounts of blood vessels supplying it, the amount of dye which is seen on the scan will differ between the two.
This difference on the scan allows the radiologist or surgeon to determine where and what the tumour is.
The surgeon may also order some blood tests, including blood tumour markers. These tests may also shed further light as to what the tumour is.
Occasionally, if all of the above are inconclusive, an endoscopic ultrasound may need to be performed. This is an endoscope, placed through the mouth into the stomach and the first part of the small bowel. What is special about this scope is that it has an ultrasound at the tip of it, allowing the pancreas to be scanned at a close distance, giving excellent quality images. Furthermore, biopsies can be taken if necessary.
What is the treatment for pancreatic lesions?
The treatment of a pancreatic lesion depends entirely upon the nature of it and how certain we can be as to what it is. Sometimes, an operation may be necessary; sometimes we can watch and wait. Occasionally, other treatments such as chemotherapy may be recommended.
In cases where there is uncertainty as to what the lesion may represent, cases should be discussed at a multidisciplinary meeting where radiologists, surgeons and other specialists can come together to discuss difficult cases. At CESA, our surgeons are associated with multidisciplinary teams which can provide such support if required.
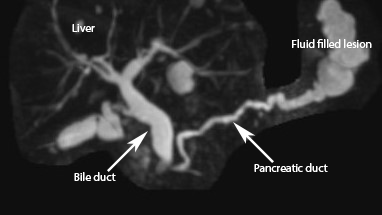
A fluid filled (cystic) lesion at the tail of the pancreas. This turned out to be an IPMN which is a precancerous lesion. The patient had a laparoscopic distal pancreatectomy (surgical removal of the tail of the pancreas) and recovered well.