
Pancreatic Resection
What is a pancreatic resection?
Pancreatic resection is the surgical removal of part of the pancreas. It is also known as a “pancreatectomy”. The most common reason why one might want to undergo this procedure is for the treatment of a pancreatic tumour.
What does a pancreatic resection involve?
As described in the section on pancreatic cancer, the pancreas is an elongated organ which runs from the just to the right of the midline to the left upper abdomen. On the right side, it hooks around some large blood vessels supplying the liver and also lies on the common bile duct which drains bile from the liver and is wrapped around the side by the first part of the intestines (the duodenum). On the left side, it touches the spleen. Due to these differences in the structures surrounding the pancreas, the left and right sided operations are very different.
Left sided pancreatic resection – Distal Pancreatectomy
This is an operation which involves the removal of the left (tail) part of the pancreas. This operation can be performed either as an open or laparoscopic (keyhole) procedure. Depending on the suspected diagnosis of the tumour as well as its location, one may preserve or remove the spleen at the same time.
Essentially, the operation involves isolating the part of the pancreas, controlling its blood supply and then cutting that part of the pancreas off. As the pancreas is cut, there is a risk of leakage of pancreatic juices from the cut surface. This is an important complication of the operation (see Complications section).

(a) (b)
Caption: Distal pancreatectomy involves the removal of the tail of the pancreas (with or without the spleen). This is illustrated in (a) with the removed parts being in grey. (b) shows what remains after distal pancreatectomy.
Right sided pancreatic resection – Whipple or Pancreaticoduodenectomy
This is an operation which involves the removal of the head (right part) of the pancreas. This operation is generally performed as an open procedure, although in certain cases at least part of the operation can be performed laparoscopically (keyhole surgery).
Due to the location of the head of the pancreas and the fact that it is surrounded by a lot of important structures, this is a much more complex operation. It involves also the removal of part of the small intestine (duodenum), part of the stomach, part of the bile duct as well as the gallbladder. After their removal, the second part of the operation involves reconnecting all these structures together so that one can eat and digest food again. Just as changing the household plumbing can lead to leaks at the joins, the most dreaded complications associated with this operation are leaks from any of the three joins (see Complications section).
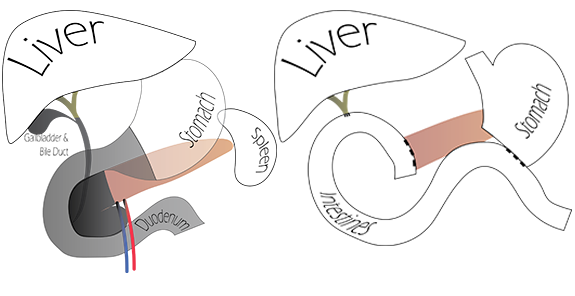
Caption: A whipple procedure (for head of pancreas tumours) involves the removal of the gallbladder, part of the bile duct, part of the stomach, the duodenum and of course the head of the pancreas. These areas are highlighted in grey in (a). (b) shows the reconnection of the bile duct, the stomach and the pancreas to the intestine so that one can eat and digest food again.
Total pancreatectomy
This is not as commonly performed as the above. It is basically an operation which combines the above two operations. As such, it is a complex operation. Furthermore, as the pancreas is completely removed, one will need to use medications to take over the function of the pancreas. Specifically:
- As there is no insulin secretion, diabetes will occur. Patients will therefore need to take insulin injections.
- As there is no secretion of pancreatic enzymes which are essential for food digestion, patients will therefore need to take regular enzyme supplements with their meals.
Abandoning resection
At the start of any of the above operations, the surgeon first looks for evidence of spread of cancer. Sometimes the spread of pancreatic cancer is too small to be detected by scanning and is only obvious at operation. In these cases, a biopsy will be taken at the operation and the operation may be stopped at that point.
At other times, the tumour may be found to be more advanced than expected and that safe removal of it would appear impossible (unresectable). In these cases, the operation may also be stopped. It is important to appreciate that if surgery proceeded regardless of spread or “unresectability”, the patient will be subjected to unnecessary risk with no real benefits. Rather, by stopping the operation, the patient will have a better chance of being well enough for other therapies such as chemotherapy.
Whilst none of the above operations are to be undertaken lightly, for pancreatic cancer or other potentially cancerous tumours, performing such an operation offers the best survival. Importantly however, pancreatic surgery is not like hernia or gallbladder surgery – each patient’s situation is different and requires careful consideration by the surgeon (in conjunction with a multidisciplinary team of specialists) regarding the pros and cons of surgery. The information described here is generic and does not replace careful discussions with your surgeon regarding the risks and expected outcomes of surgery.
What are the risks of surgery?
Like any operation, there are risks. As these operations are all major operations, the risks are very significant.
Firstly, there are risks associated with the anaesthetics – this is related to the patient’s age and medical issues. In general, due to the nature of the surgery, the patient will be booked in for the preadmissions clinic where the patient will see the anaesthetist to have these risks assessed and fully explained. To help manage these risks, patients are generally transferred to the High Dependency Unit or Intensive Care Unit for the first few days after the operation for intensive monitoring.
With regards to surgical risks, the specific risks of surgery include:
- Pancreatic leak – this is a feared complication from pancreatic surgery. The exact risk of this varies depending on many factors, but occurs in more than 1 in 10 patients. In surgery of the tail (distal pancreatectomy), the leak arises from the cut end of the pancreas; in a Whipple procedure (head of pancreas), the leak arises from the join to the bowel. Leakage in a Whipple procedure is particularly concerning as the pancreatic juice may be in an activated form (activated by substances in bile) and so may cause digestion and damage to surrounding structures. The treatment of this varies: medications, drainage, endoscopy or reoperation.
- Leakage at other joins – The Whipple procedure involves joins of the bile duct as well as the stomach to the small intestines. Although less common than pancreatic leakage, these can nonetheless occur. Treatment may involve either putting in a drain tube or reoperation.
- Bleeding – Due to the intimate closeness of the pancreas with many major blood vessels, major bleeding may occur. This may sometimes be managed by blocking off the artery by an injection, but may sometimes require a reoperation.
- Ileus or delayed gastric emptying – The function of the stomach and the intestines are impaired after this type of major operation and may not return to function for many days. This may cause vomiting and bloating of the abdomen and failure to absorb nutrition given by mouth. As a consequence, nutrition through the drip (“TPN”) may be required.
- Pancreatic insufficiency – removal of part of the pancreas may mean that the patient won’t have enough functional pancreas to produce insulin and digestive enzymes. This may result in diabetes and malabsorption. These may require treatment with insulin and pancreatic enzyme supplementation.
- Death – Like any major surgery there is a risk of dying at or after the operation. The risks are greater with a head operation (Whipple operation) but should be less than 1 in 20. The risks of death in a tail operation (Distal pancreatectomy) is in the order of 1 in 100.
- Other general complications of major surgery such as wound or deep infections, clots in the legs of lungs, urinary or chest infections, adhesions (scarring inside) and hernias may occur also.
I am having surgery for the pancreas, do you have any further information regarding this operation?
Yes. We have created an information sheet for our patients undergoing pancreatectomy. Do note that this is generic information and may not apply specifically to your circumstance.
If you are undergoing surgery with us at CESA, our surgeons will explain everything to you in detail with information which is tailored to your specific circumstances. Also, feel free to ask your surgeon any questions which may not be covered in the information sheet.