
Piles and Haemorrhoids
What are Haemorrhoids?
Haemorrhoids are engorged blood vessels covered by the lining of the anal canal that may slide down (prolapse), enlarge or bleed.
Prevalence
- About 4-5% of population have haemorrhoidal problems
- Only 1/3 will go to see a doctor
- It usually affects people in the age group 45-65 years. The prevalence decreases after 65 years of age
- It rarely affects people under 20 years of age
What causes Haemorrhoids?
- Haemorrhoids are associated with straining and an irregular bowel habit, especially constipation.
- Hormonal changes during pregnancy predisposes to the development of haemorrhoids or can lead to exacerbation of pre-existing haemorrhoids.
What are the symptoms of Haemorrhoids?
- Bleeding – Typically, this is bright red, painless and occurs at the end of defaecation. The bleeding is often described as blood on the paper, dripping or spraying into the toilet bowl. The bleeding may also be “hidden”, i.e. tested positive on stool test (Faecal Occult Blood Test) but not visible on inspection. It is very important not to assume all bleeding are due to haemorrhoids. Bowel cancer can give rise to bleeding as the only symptom. Therefore, it is essential to exclude other causes of bleeding first before attributing bleeding to haemorrhoids. Investigations for bleeding may include flexible sigmoidoscopy or colonoscopy.
- Anaemia – With prolonged history of bleeding, the patient may become anaemic. The recovery from anaemia after haemorrhoidectomy is usually rapid.
- Prolapse – This usually occurs during straining at the time of defecation. In the majority of situations, the haemorrhoids reduce by themselves. Occasionally, they need to be pushed back in. When the haemorrhoids become very large, they are not reducible and they stay out of the anus all the time.
- Pain – Pain is not a symptom of uncomplicated haemorrhoids. It may indicate other diseases such as an abscess or anal tear (anal fissure). Painful haemorrhoids are uncommon and they are usually a result of thrombosis (clotting) or strangulation (prolapse leading to obstruction of blood flow in and out of the haemorrhoid).
- Itchiness (pruritus ani) – This is related to mucous leakage which can lead to itchiness and a burning discomfort in the skin around the anus.
Treatment of Haemorrhoids
Non-Operative Treatment
- High fibre diet
- Fibre supplement such as Metamucil, Benefibre, Normacol or Fybogel
- Must not ignore the urge to open bowel.
Minor Operative Procedures
Banding of haemorrhoids consists of putting rubber bands over the haemorrhoids to cut off their blood supply. This leads to the shrinkage of the haemorrhoids and they drop off the bowel wall usually in 7-10 days. A maximum of 3 haemorrhoids may be ligated at any one time. This method is effective for small internal haemorrhoids.
Risks:
- Significant bleeding is rare
- Usually dull ache for 24-48 hours
- Severe pain is uncommon
- Severe infection is rare
Operative Procedures
1. Open Haemorrhoidectomy
- Necessary for large or complicated haemorrhoids
- This procedure is performed under general anaesthetic in a hospital or Day Surgery Centre
- It involves the cutting out of the haemorrhoids. A maximum of 3 haemorrhoids can be removed at any one time with careful preservation of the mucosal bridges (to prevent anal narrowing) and the identification and preservation of internal anal sphincters (to prevent faecal incontinence).
Disadvantages:
- Main disadvantage is significant anal pain for at least 2 weeks despite laxatives, analgesia, oral Metronidazole and warm baths. It occasionally needs to be performed in 2 stages if the haemorrhoids are large and circumferential
- Risks: <5% risk of bleeding requiring hospitalization or intervention, delayed wound healing (similar to an anal fissure), faecal incontinence (uncommon) and rare anal narrowing
2. Ligasure Haemorrhoidectomy
- Similar to open haemorrhoidectomy in that the haemorrhoid is excised. However, the excision is carried out using Ligasure Small Jaw rather than standard diathermy. This instrument reduces the size of the wound, postoperative pain and operating time.
- It is suitable for patients who have large internal haemorrhoids, large external haemorrhoids and/or large skin tags (4th degree haemorrhoids)

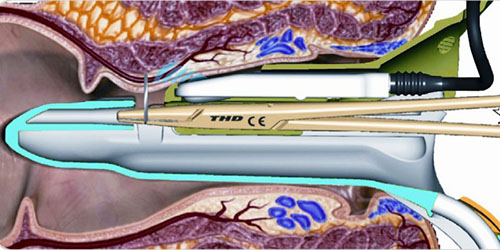
3. Transanal Haemorrhoid Dearterialisation (THD)
- In the search for a painless surgical treatment for haemorrhoid, transanal haemorrhoid dearterialisation (THD) is an innovation based on a different principle from conventional open haemorrhoid operation. Since it was first reported by Morinaga and colleagues in 1995, it has gradually gained in popularity among surgeons.
- The operation involves the use of a specifically designed proctoscope (a short instrument that inserted into the anus to provide an internal view) together with an ultrasound device. With the rotation of the proctoscope, the ultrasound allows for the detection of the branches of haemorrhoidal arteries, which are then tied off with sutures. As a result, the blood flow is reduced which lead to the shrinkage of haemorrhoids. In addition, a continuous stitch to the haemorrhoids is carried out that compresses the haemorrhoids tightly and further reduces the blood flow to the haemorrhoids. In fact, the internal haemorrhoids are removed by making them “die inside”.
- The pain from this operation is minimal because the technique avoids suturing the sensitive area inside the anus and it also avoids any external wound. Therefore, the main advantages are minimal pain after operation, minimal use of pain killers, no need to use warm/Sitz bath, a safe operation and quicker recovery (compared to open haemorrhoidectomy). The disadvantages are that it is not suitable for patients with large external haemorrhoids or in patients who would like to have their skin tags removed.
- The chance of haemorrhoids returning after this operation is about 10%. The operative risks are low incidences of bleeding and anal pain.
Dr Chew believes THD is effective in controlling symptom of rectal bleeding especially in patients who had failed banding of haemorrhoids. However, ligasure haemorrhoidectomy is a better option for fourth degree haemorrhoids (large permanently prolapsed haemorrhoids) or in those patients who have large external haemorrhoids/anal skin tags.